Musculoskeletal Complications of Radiation Therapy
Recognizing and differentiating radiation-induced injuries in the emergency setting


In concert with the RadioGraphics monograph, RSNA News shares the latest research on emergency imaging.
Up to a third of patients receiving radiation therapy (RT) or immunotherapy develop musculoskeletal complications. Many have complex clinical and imaging features that can resemble metastatic disease or infection on imaging.
"Radiation effects on bone and soft tissue evolve and vary by technique,” said Majid Chalian, MD, associate professor of musculoskeletal radiology at the University of Washington (UW) in Seattle. "The degree of post-RT bone changes depends on the patient's age, radiation dose, radiation delivery technique, and volume of irradiated tissue."
To help radiologists differentiate RT-related MSK complications, Dr. Chalian and his colleagues developed a review published in RadioGraphics identifying post-treatment imaging characteristics of various RT techniques, including conventional therapy, stereotactic body radiation therapy, 3D conformal, intensity-modulated radiotherapy and proton therapy, as well as a timeline for when they occur.
The authors identified several key variables that can influence how radiation-induced MSK injuries appear on imaging:
- Total radiation dose
- Technique and use of fractionation
- Volume of irradiated tissue
- Tissue radiosensitivity
- RT field location
- Treatment timeline
One of the study’s lead authors Arash Azhideh, MD, MPH, a postdoctoral research fellow at UW, also stressed the importance of understanding RT fundamentals, including the alpha-beta (A/B) ratio of irradiated tissue, which reflects the ability to repair damage between treatments. Low A/B ratio tissues show delayed chronic effects, while high A/B ratio tissues show early acute ones.
"With the increasing use of altered fractionation, radiologists should be aware that imaging findings will reflect the effective dose rather than the total dose delivered,” Dr. Chalian added.
Understanding these factors helps radiologists recognize the earliest imaging signs of MSK injury.
Identifying MSK Complications
Acute and delayed MSK complications include bone fragility, insufficiency fractures, osteoradionecrosis, inflammatory arthritis, myositis and tendinopathy.
The most common complication of irradiated bones is fracture, with the pelvic bone, sacrum and spine being most prone. Post-RT bone may appear normal on radiographs initially, but can reveal osteopenia, sclerosis and coarse trabeculation one-year post-treatment. Impaired vascularity may further weaken bones, increasing the possibility of fractures.
"Insufficiency fractures may mimic a tumor recurrence," Dr. Chalian said. "When describing bone changes post RT, radiologists should focus on recognizing hallmark imaging features of the bone injury rather than the location, extent and chronicity."
Non-degenerated cartilage has traditionally been considered relatively resistant to radiation, with the notable exception of pediatric patients. Nonetheless, RT can induce significant changes in adjacent soft tissues and muscle, including fibrosis, edema, atrophy, and fatty replacement within the irradiated field.
Dr. Chalian noted that among soft tissue sarcomas, undifferentiated pleomorphic sarcomas and angiosarcomas are the most frequently reported malignancies associated with prior radiation exposure. These observations underscore the importance of careful tissue assessment and long-term surveillance following RT, particularly in high-risk populations.
Being aware of the patient's history and knowing how much time has transpired between the start of treatment and the imaging study is critical for identifying MSK complications.
"Without that context, diagnosis can be challenging and result in unnecessary interventions. Different post-treatment time spans result in specific types of complications," Dr. Chalian said.
But knowing when complications tend to appear is only part of the challenge. According to the authors, a big pitfall in interpreting post-treatment MSK complications is differentiating a recurrent or residual tumor from an infection.
"In addition to knowing what complications can happen after radiation or immunotherapy and what to look for, it takes practice to be able to distinguish complications from other findings," Dr. Chalian said.
MSK RT complications may mimic other conditions, such as inflammatory arthritis, polymyalgia rheumatica, myositis, tenosynovitis and bone marrow reactivation.
"Inflammatory conditions such as fasciitis and myositis, and complications including osteonecrosis, fractures and lymphedema are among the biggest diagnostic challenges for radiologists when reviewing post-treatment imaging,” Dr. Azhideh said.
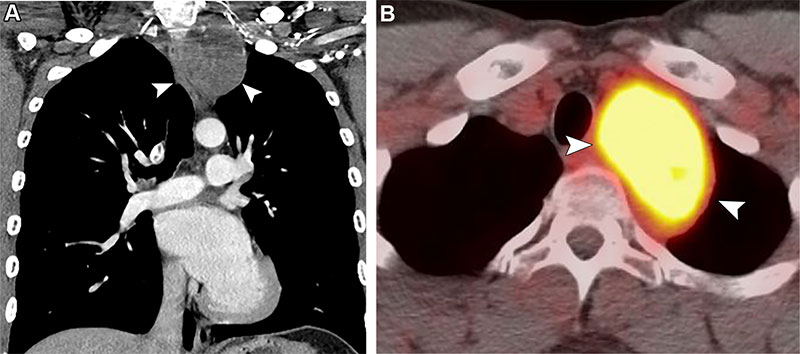
Post-RT malignancy in a 27-year-old man with a history of treated Hodgkin lymphoma and RT 12 years earlier. Coronal CT (A) and axial FDG PET/CT (B) images show a well-defined mass (arrowheads) in the left upper mediastinum demonstrating intense FDG uptake without evidence of osseous invasion. Histopathologic examination results revealed a malignant peripheral nerve sheath tumor.
https://pubs.rsna.org/doi/10.1148/rg.250014 ©RSNA 2025
Recognizing Immunotherapy’s MSK Risks
While RT-related MSK injuries have been well-documented, newer cancer treatments such as immunotherapy present a different spectrum of complications.
Newer immunotherapies, particularly immune checkpoint inhibitors, have distinct immune-related MSK toxicities that can occur with other systemic side effects. The most common MSK complication of immunotherapy is arthralgia, followed by arthritis and synovitis. Fractures involving the spine, hip and femur are also common. These can mimic conditions like inflammatory arthritis, polymyalgia and myositis.
"Because immunotherapy is relatively new, patients undergoing this treatment may present with complications that radiologists are not well-versed in,” Dr. Chalian said. “Recognizing these complications in their clinical and imaging contexts is critical for accurate diagnosis, prompt treatment and better patient outcomes.”
Unlike RT, in which complications are confined to the boundaries of radiation and may occur years after treatment, immunotherapy complications may be systemic and more immediate. For example, an MRI of a patient who develops wrist pain while undergoing immunotherapy may reveal tenosynovitis.
"Correctly identifying it as a complication of immunotherapy means we can prevent further investigation, such as a biopsy or unnecessary treatments," Dr. Chalian said. “Informing the patient's physician of MSK complications may also result in a modulation of the immunotherapy dose, reducing its effects.”
Treatment regimens are also beginning to combine RT and immunotherapy. Dr. Azhideh cited evidence that when used together, they have synergistic effects. "However, the combined therapy may increase the rate of complications," he said. “Many immunotherapy drugs are still in clinical trials, but some, such as treatments for blood, skin and other cancers, are being approved for daily practice.”
By providing valuable information on the characteristics of RT-related MSK complications, the RadioGraphics article and further research will not only benefit cancer patients post-therapy but can also inform treatment planning.
“With new radiation delivery techniques and new forms of immunotherapeutic drugs in development, ongoing investigation will allow continued refinement of the imaging criteria of early complications and improvement is patient care,” the authors conclude.
For More Information
Access the RadioGraphics article, “Musculoskeletal Complications of Radiation Therapy and Immunotherapy.”
Read previous RSNA News stories on complications of radiation therapy: