Patients with HIV Face Increased Cardiovascular Risk as They Age
CT characterization of noncalcified coronary plaque helps predict future cardiovascular risk

As people with HIV live longer, they are more frequently subjected to age-related diseases, such as coronary artery disease. In fact, those without known cardiovascular disease, have two to three times the noncalcified coronary burden of non-HIV healthy volunteers, according to a Radiology study.
Study lead author Carl Chartrand-Lefebvre, MD, MSc, professor and chairman in the Department of Radiology, Radiation Oncology and Nuclear Medicine, University of Montreal, and his colleagues sought to understand the relationship between HIV and increased risk of cardiovascular disease.
“In 2011, Dr. Cécile Tremblay, a microbiologist and HIV specialist in Montreal needed a noninvasive approach for the assessment of cardiovascular disease as part of a prospective cohort of people living with HIV she was following,” Dr. Chartrand-Lefebvre said. “HIV specialists like her were aware of a significant shift in the causes of mortality in people living with HIV, with more and more individuals in the HIV population afflicted by an increasing rate of myocardial infarction.”
At the same time Dr. Tremblay’s group reported an increased risk of myocardial infarction in this group of individuals, researchers in the U.S. and France were reporting similar tendencies.
Small Pilot Study Yields Suboptimal Result
“It was becoming urgent to evaluate the determinants of the evolving causes of mortality and morbidity in the ever increasing, aging HIV population, especially in the preclinical stage of cardiovascular disease,” Dr. Chartrand-Lefebvre said.
Drs. Tremblay and Chartrand-Lefebvre agreed to use cardiac CT as the modality of choice to investigate coronary artery atherosclerosis (CAD) in asymptomatic people living with HIV. They began a small pilot study intended to allow preliminary results they hoped would lead to a grant application for a multicenter prospective study.
They used non-contrast CT in 78 people living with HIV over the age of 40 who had no CAD history or symptoms. The subjects had intermediate risk for CAD according to the 10-year Framingham cardiovascular risk score (FRS) in comparison to non-HIV individuals, matched 1:1 for age, gender and FRS.“It was becoming urgent to evaluate the determinants of the evolving causes of mortality and morbidity in the ever-increasing aging HIV population, especially in the preclinical stage of cardiovascular disease.”
CARL CHARTRAND-LEFEBVRE, MD, MSc
Possibly due to its small size, the pilot study showed no difference in coronary calcium prevalence and scores between the two groups.
“We concluded, as others had, that calcium detection with non-contrast CT may not be the optimal approach in the HIV population, at least in young adult patients, since calcium deposition occurs late in the pathogenesis of CAD,” Dr. Chartrand-Lefebvre said.
Coronary CT Angiography, A More Suitable Modality
To take a second attempt at their hypothesis, the researchers started prospective recruitment of both asymptomatic people living with HIV and healthy volunteers without HIV or known cardiovascular disease as part of the Canadian HIV and Aging Cohort Study (CHACS), a prospective, controlled cohort study funded by the Canadian Institutes of Health Research.
They performed CT angiography assessment on their first study sample of 265 participants: 181 people living with HIV and 84 healthy volunteers. The results showed no difference between the two groups in coronary artery calcium score and overall plaque prevalence.
However, noncalcified coronary plaque prevalence and volume were two to three times higher at coronary CT angiography in asymptomatic people living with HIV without known cardiovascular disease than in healthy volunteers without HIV.
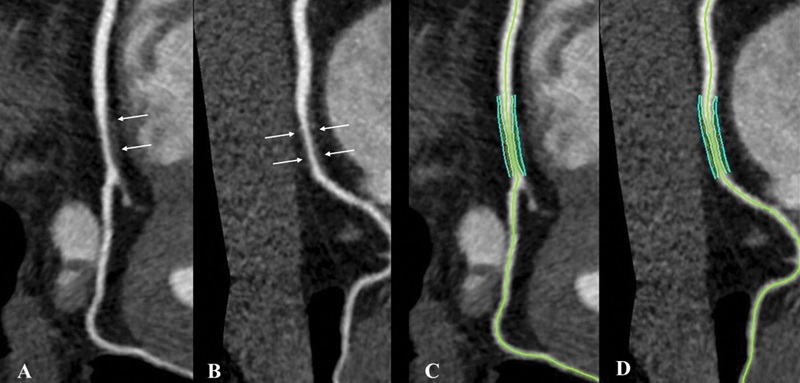
Noncalcified coronary plaque in an asymptomatic 52-year-old man living with HIV with a 10-year Framingham risk of 5%. Images show 256-section contrast-enhanced coronary CT angiography with electrocardiographic gating and curve reformat. A, B, CT scan shows a smooth noncalcified plaque in the right coronary artery (arrows) with 70%–80% stenosis. C, D, The right coronary artery plaque volume was 130 mm3 (cyan lines).
Boldeanu et al, Radiology 2021; 299:571–580 ©RSNA 2021
“For radiologists, these results suggest that coronary CT angiography interpretation in people living with HIV should probably include quantification of coronary plaque by subtypes to allow better cardiovascular risk stratification,” Dr. Chartrand-Lefebvre said.
Despite using epidemiological research standards to minimize between-group disparities and ensure representation in their patient sample, the team encountered differences for gender and smoking history, both factors in cardiovascular risk. They used multivariable models to reduce the effects of these confounders.
“Another limitation was that the proportion of women in our study, at 8%, does not mirror the sex distribution of the HIV epidemic in Canada which is 22% women,” Dr. Chartrand-Lefebvre said. “In the future, we intend to collaborate with the University of British Columbia in Vancouver where there is a clinic dedicated to care of women living with HIV.”
He and his fellow researchers have begun performing repeat studies in participants who already underwent a first CT study as part of the CHACS. Their plan is to allow a longitudinal assessment of the evolution of subclinical coronary atherosclerosis and to observe the parameters that might influence the characteristics of the plaque burden changes.
In addition, the team is using CT to assess epicardial fat and muscular mass, using muscular mass measurement to correlate with clinical assessment of frailty, as part of graduate student research programs. They are also using US and quantitative carotid elastography to evaluate subclinical carotid atherosclerosis, under the lead of Guy Cloutier PhD, professor of radiology, radio-oncology and nuclear medicine, Université de Montréal and the Research Center of the CHUM.
Dr. Chartrand-Lefebvre noted that as part of their ongoing research activities, the team is collaborating with the research teams of the laboratories of immunovirology in the CHACS, in University of Montreal, McGill University and Université du Québec à Montréal, to identify inflammatory markers within the imaging data.
WEB EXTRAS
Access the Radiology study, “Prevalence and Characterization of Subclinical Coronary Atherosclerotic Plaque with CT among Individuals with HIV: Results from the Canadian HIV and Aging Cohort Study.”
Read previous RSNA News stories about cardiovascular risk: