Quantitative Dynamic MRI Shows Promise for Children with Thoracic Insufficiency Syndrome
AI-powered technique may apply to wider population of respiratory ailments

A quantitative dynamic MRI (QdMRI) method shows promise for treating children with Thoracic Insufficiency Syndrome (TIS), a rare, potentially lethal disease of the spine that prohibits the thorax from supporting normal breathing or lung growth, according to new Radiology research.
Patients with spinal and chest wall deformities are assessed by measuring the degree of scoliosis and determining lung volumes using pulmonary function testing. Although there is a variable correlation between these measures in patients with such disorders as adolescent idiopathic scoliosis, the correlation is poor in patients with TIS.
With abnormal lung growth impairing the respiratory function, TIS often leads to respiratory failure and an increased risk of early death. TIS, which affects fewer than 4,000 children in the U.S., is associated with a wide variety of diseases and conditions, including cerebral palsy, spina bifida, congenital scoliosis and spinal muscular atrophy.
“A reconstructive spine and chest wall operation can be performed in growing children with TIS when there is a progressive thoracic deformity that may limit future lung development or thoracic function,” said Harriet J. Paltiel, MD, Boston Children’s Hospital and Harvard Medical School and author of a recent Radiology editorial on the topic. “However, there is currently no widely accepted and validated outcome measure to assess postoperative changes in respiratory function in patients with TIS.”

This could soon change. In the Radiology study, a joint team from the Medical Image Processing Group of the University of Pennsylvania, headed by study author Jayaram K. Udupa, PhD, and the Center for Thoracic Insufficiency Syndrome at the Children’s Hospital of Philadelphia, headed by Patrick J. Cahill, MD, has developed and validated a QdMRI method to compare the regional dynamics of the lungs, chest wall, and hemi-diaphragms in children with TIS, before and after surgical treatment.
“As patients with TIS have extreme difficulty breathing normally, it is impossible to have them cooperate with imaging techniques that require them to hold their breath,” said Dr. Udupa, radiology professor and chief of the Medical Imaging Section at the University of Pennsylvania. “That is why our QdMRI technology, which we are developing for routine clinical use, is based on free-breathing dynamic MRI and advanced artificial intelligence (AI) powered image analysis.”
Study Highlights
- Images from free-breathing dynamic MRI in pediatric patients with TIS (July 2009–August 2015) were retrospectively evaluated before and after surgical correction by using vertical expandable prosthetic titanium rib (VEPTR).
- Four-dimensional image construction was performed by obtaining a subset of the two-dimensional free-breathing dynamic MRI sections, which represents one four-dimensional volume over one respiratory cycle.
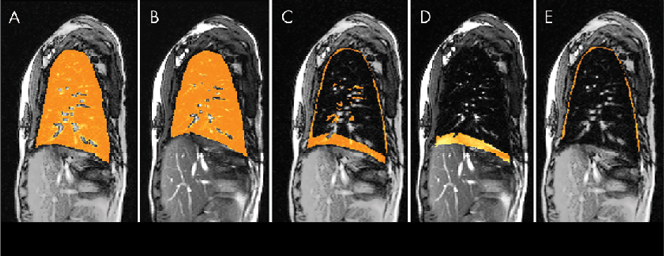
- The left and right lungs were then separately segmented in the four-dimensional volume at end inspiration and end expiration.
- By subtracting end-expiration images from end-inspiration images for each lung, lung excursion difference images are created, from which the chest wall and diaphragmatic components of lung excursion are derived separately.
“This marking operation is currently done manually, which typically consumes about four hours of human time to examine all 2,000-3,000 slices and determine which slices correspond to end expiration and end inspiration time points,” Dr. Udupa said. “Our AI-based auto-labeling method reduces the human time required to 10-15 minutes per dMRI study and provides comparable accuracy to manual labeling.”
Study Results
Using QdMRI to depict changes in regional dynamic thoracic function before and after surgical correction of TIS shows that:
- Average left and right lung volumes at end inspiration and end expiration increased substantially after an operation.
- Average lung tidal volume (i.e., the standard volume of air displaced between normal inhalation and exhalation when extra effort is not applied) improves.
“This technique holds promise for improving our ability to accurately document the functional results of VEPTR in patients with TIS, and it may apply to a wider population of patients with impaired respiratory function associated with spinal and chest wall deformities,” Dr. Paltiel said.
Read the full story in the September print issue of RSNA News.
For More Information
Access the Radiology editorial, “Can Dynamic MRI Depict Change in Thoracic Function after Operation for Thoracic Insufficiency Syndrome?” and the Radiology study, “Quantitative Dynamic Thoracic MRI: Application to Thoracic Insufficiency Syndrome in Pediatric Patients.” Within the Radiology study, access videos showing 4D animation of the lung dynamics of a patient with neuromuscular scoliosis and Thoracic Insufficiency Syndrome.
Access the 2018 study, “Lung Parenchymal Analysis on Dynamic MRI in Thoracic Insufficiency Syndrome to Assess Changes Following Surgical Intervention,” by Dr. Udupa and colleagues at SPIEDigitalLibrary.org.