MR Scoring Algorithm Can Help Radiologists Determine Next Steps for Renal Masses
Score can prevent over-treatment of renal masses

For patients with small indeterminate solid renal masses, a new MR imaging assessment score shows potential in predicting aggressive malignancies—and it’s easy for radiologists to learn with minimal training.
The clear cell likelihood score (ccLS), developed by researchers at the University of Texas (UT Southwestern) Medical Center in Dallas, targets clear cell histology, the most common malignancy and one that commonly exhibits aggressive behavior among renal masses.
Historically, the only way to inform the risk of aggressive histology in renal masses was with a biopsy, according to Ivan Pedrosa, MD, PhD, professor of radiology and urology and vice-chair of research in the Department of Radiology at UT Southwestern Medical Center. The score, evaluated during a multicenter trial described in a recent Radiology study, was developed to help radiologists diagnose clear cell histology noninvasively.
“The management decisions for an indeterminate solid renal mass are multifactorial and are influenced by its size, patient factors such as comorbidities, age and life expectancy, and patient preference,” explained Dr. Pedrosa, who is also the Jack Reynolds, MD, Chair in Radiology and co-leader of the Kidney Cancer Program at the Harold C. Simmons Comprehensive Cancer Center at UT Southwestern. “However, up to one in five small renal masses are benign—and when malignant they may exhibit an indolent behavior. Thus, current management strategies that promote definitive therapy are arguably leading to over-treatment of renal masses, particularly in older patients with limited life expectancy.”
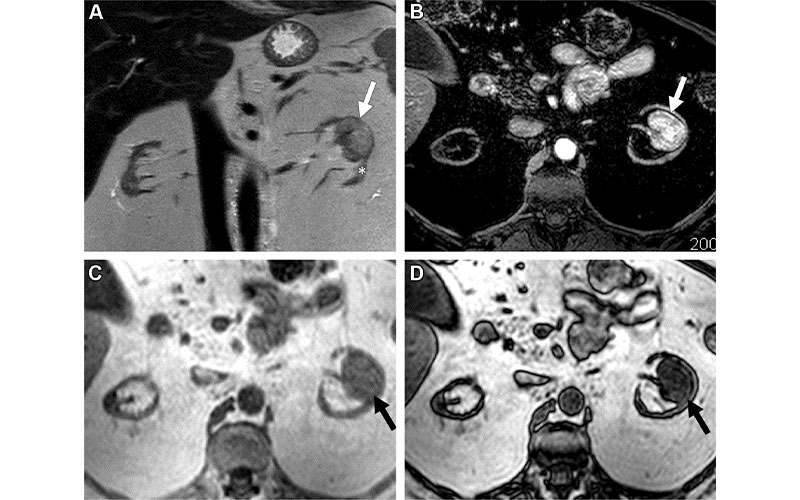
MRI scans in a 56-year-old woman with an indeterminate 3.2-cm left renal mass (arrow). (A) Coronal T2-weighted single-shot fast spin-echo image shows a left renal mass with heterogeneous signal intensity greater than that of the adjacent renal cortex (*). Note severe atrophy of both kidneys due to end-stage renal disease. (B) Axial fat-saturated T1-weighted spoiled gradient-echo image acquired during the corticomedullary phase after gadobenate dimeglumine administration (0.1 mmol per kilogram of body weight) shows intense heterogeneous enhancement that is higher than that of the adjacent renal cortex. Quantitative analysis demonstrated more than 75% enhancement in the renal mass compared with the renal cortex. (C, D) Axial T1-weighted gradient-echo in-phase (C) and opposed-phase (D) images show unequivocal presence of microscopic fat in the mass, with an apparent decrease in signal intensity in D compared with C. Both reviewers assigned a clear cell likelihood score of 5 in this mass. After nephrectomy, a diagnosis of clear cell renal cell carcinoma was confirmed.
Schieda et al, Radiology 2022; 303:590–599 ©RSNA 2022
Likelihood of Clear Cell Renal Cell Carcinoma Identified with ccLS Score
The ccLS utilizes the imaging characteristics of a renal mass on multiparametric MR imaging to assess the likelihood of that mass representing clear cell renal cell carcinoma.
Dr. Pedrosa’s team used three major criteria for the score: The predominant signal intensity of the enhancing component of the mass on T2-weighted images, the maximum enhancement during the corticomedullary phase after contrast administration, and the presence of microscopic fat on in-phase/opposed-phase MR imaging.
“Once those have been evaluated, the final ccLS is then assigned using additional ancillary features such as the arterial-to-delayed enhancement ratio, marked restriction on diffusion weighted imaging, and the presence of segmental enhancement inversion,” Dr. Pedrosa said.
For their study, the researchers included 241 patients and focused on small renal masses—4 centimeters or smaller in diameter. They found that the ccLS algorithm produced moderate sensitivity for diagnosis of clear cell renal cell carcinoma as well as promising negative predictive value.
“Although the ccLS does not inform about the likelihood of the mass being cancer—instead, it informs about the likelihood of a mass representing a clear cell renal cell carcinoma—certain scores and imaging features enable reporting a higher likelihood of a renal mass being benign,” Dr. Pedrosa explained. “For example, a high likelihood of lipid-poor angiomyolipoma or oncocytoma may be suggested with the right combination of imaging findings.”
“Up to one in five small renal masses are benign—and when malignant they may exhibit an indolent behavior. Thus, current management strategies that promote definitive therapy are arguably leading to over-treatment of renal masses, particularly in older patients with limited life expectancy.”
IVAN PEDROSA, MD, PhD
Radiologists Can Use ccLS to Begin Identifying Predictive Parameters
The team was pleasantly surprised to find that, after only an hour and a half of training, abdominal radiologists with no previous experience using the ccLS were able to replicate the single-center early experience at UT Southwestern, Dr. Pedrosa noted. However, the researchers observed discrepancies in diagnosis when they examined individual predictive parameters.
“We need to understand better what may have influenced these results and, if appropriate, further refine the ccLS algorithm,” Dr. Pedrosa said.
Achille Mileto, MD, and Theodora A. Potretzke, MD, both of the Mayo Clinic, Rochester, MN, discussed the clinical merits of the ccLS in an accompanying Radiology editorial, touting its potential to provide a framework for assessing small solid renal masses with MR.
Drs. Mileto and Potretzke noted that ccLS could help to establish a standardized process for evaluating masses across imaging facilities, as well as support informed decision making for treatment planning.
“One future direction may be to account for the diagnostic challenge often posed by oncocytomas and oncocytic-spectrum lesions (including hybrid oncocytic-chromophobe neoplasms), which often do not show any specific diagnostic features and are indistinguishable from RCCs, particularly the chromophobe subtype,” the authors wrote.
It may also be employed to identify other aggressive features, such as the sarcomatoid phenotype—a histologic differentiation of renal cell carcinoma that’s not designated as a distinct histotype but that can be observed with any subtype, they observed.
For More Information
Access the Radiology study, “Multicenter Evaluation of Multiparametric MRI Clear Cell Likelihood Scores in Solid Indeterminate Small Renal Masses,” and the accompanying editorial, “Standardized Evaluation of Small Renal Masses Using the MRI Clear Cell Likelihood Score.”
Read previous RSNA News articles on abdominal and renal imaging: